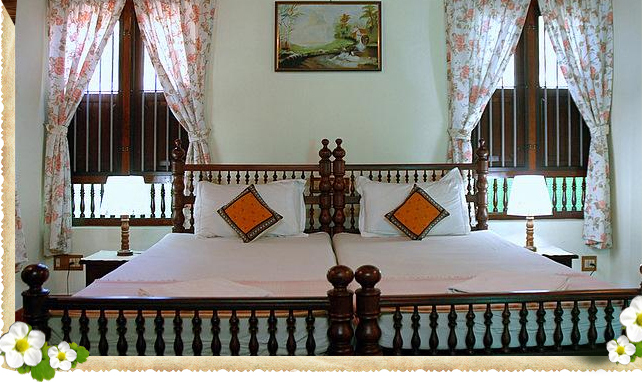
Cochin Heritage Home situated in the heart of the historic and picturesque township of Fort Cochin, welcomes you as our honored guest at any time of the year. We are located near the Bishop’s House, a prominent landmark. Other structures having tourist interest, such as the St. Francis Church, the Dutch Palace, Chinese fishing nets, the 500 – year old Santa Cruz Basilica, are located at points within short walking distances away. Hence, you will find Cochin Heritage Home an ideal place to stay.
Read more